

Nuclear Detonation Preparedness, PCR and Endotoxin Cytokine Storm Expert - Susan Monarez tipped to head US CDC
Very timely as Australian Warmongers sign us up to AUKUS Nuclear Submarines

I wrote about Donald Trump appointing Gerald Parker as new Director of the White House Office of Pandemic Preparedness and Response Policy, who is also an expert in Nuclear Genocide.1
And I pointed out North Korea, worried about AUKUS submarines off its coast, is capable of wiping out any Australian city with its ICBMs.2
Now let’s look at Susan Monarez who is a major Jab promoter as well as planner for dealing with millions of Americans hit by a Nuclear attack.

You might like to follow her on X and look at her posts as Acting CDC Director since 20 January 2025. It would appropriate for her to replace Endotoxin expert Fauci.3
Useful biography of Susan Monarez here.4
Look at her work in the Office of Preparedness and Emergency Operations (OPEO).
She was credited in 2011 a paper published in the journal Disaster Medicine and Public Health Preparedness.5
The paper considered an unrealistic small scale terrorist attack, rather than a modern nuclear warhead in the Megatonnes equivalent. But it matches an accidental release from one of the Nuclear Power plants proposed for Australia by Dutto, Clive Palmer and his Trumpeters, Gerard Rennick and other lunatic fringe, or an AUKUS nuclear powered submarine reactor leak as ordered by Scott Morrison and pursued enthusiastically by Albo, Marles, Wong and Chalmers who delivers his Federal Budget this evening.
A terrorist nuclear detonation of 10 kilotons would have catastrophic physical, medical, and psychological consequences and could be accomplished with a device in a small truck. Tens of thousands of injured and ill survivors and uninjured, concerned citizens would require medical care or at least an assessment and instructions. In proximity to the incident location, there would be a huge imbalance between the demand for medical resources and their availability.
Beyond the immediate blast area, much of the infrastructure would remain intact. Most people would reach medical care by selfreferral and require sorting and assessment to determine what medical intervention is necessary, appropriate, and possible.
Ethical Considerations
With the magnitude and suddenness of a nuclear incident, responders will be forced to operationalize medical triage that places many people who would normally receive first priority for care (immediate) into a category in which they will not receive “curative” treatment (expectant).
Even medicines for symptom relief may not be available, so vast numbers of casualties may receive little or no care. Rationing of medical care will be required in a context of incomplete situational awareness.
Providers will make difficult allocation decisions without the benefit of an administrative structure that could address broader optimization of resource use.
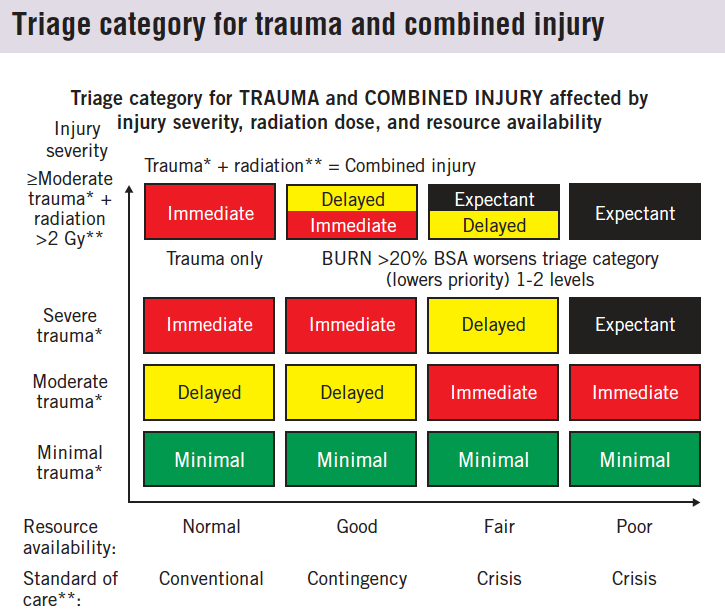
Legend: Trauma and combined injury
*Adding >20% total body surface area burn to trauma worsen triage priority by 1 category (puts them lower on the priority list).
**Radiation dose received by the whole body or a significant portion of the whole body. At higher radiation doses (>6 Gy), triage category may worsen–as on Combined Injury card.
***Institute of Medicine. Guidance for establishing crisis standards of care for use in disaster situations: A letter report. Washington, DC: Institute of Medicine, National Academies of Science; 2009.
Combined injury
• Radiation dose of >2 Gy to whole body or significant portion of whole body plus moderate or severe trauma and/or burn injury.
Severe trauma
• Stabilization requires complex treatment;
• >20% chance of death even with treatment.
Moderate trauma
• Without stabilization, potential for death within hours
• <20% chance of death with stabilization and treatment.
Minimal trauma
• Injuries pose no significant risk to life and limb in next 3-4 days
• Limited or no treatment prior to referral in the next 3-4 days.
This is 1 of a series of “cards” that indicates how triage category changes based on the availability of resources for trauma and combined injury. These are discussed in detail in Coleman et al,22 and PDFs of all cards can be downloaded at http://www.dmphp.org. There are 4 resource settings (adapted and modified from the Institute of Medicine2): normal, with conventional standards of care; good, with contingency standards in which substitution of resources allows normal triage order; crisis, which is subdivided into fair, when there are enough resources to treat the moderate life-threatening trauma, and poor, when there are insufficient resources to treat the moderates. The injury severity categories are severe life threatening, in which likelihood of death is 20% even when aggressive treatment is available21; moderate life threatening, in which the injuries are less severe and mortality is 20%; minimal, in which the injuries may require intervention, even substantial intervention, but are not life threatening within the next day or so (eg, certain limb fractures); and combined injury, which is moderate or severe life-threatening injury plus a radiation dose of 2 Gy (lower doses are not considered to be combined injury and are triaged as trauma only). Burns of 20% total body surface area worsen triage category 1 level (eg, delayed to expectant). In the conventional and contingency settings, the usual “sickest first” order is followed by severe receiving immediate care, then moderate, and minimal after that (although in a mass casualty setting, some of the minimal may be given temporary remedies and sent on for definitive care, as with a splint or bandage for fracture or non–life-threatening wound).
In the crisis setting with fair resources, moderates would be treated before severes; with poor resources, moderates would be treated first, recognizing there are not even sufficient resources for them. In general, individuals with combined injury would be treated similarly to the severe, although at the higher radiation doses survival is so limited that they may receive a lower priority (eg, in crisis, fair resources delayed may be changed to expectant). Reevaluation is a key part of triage and management because the initial triage category may change over time (eg, a moderate may become a severe) and as resource setting improves (eg, a delayed may become an immediate).
Of course the paper does not mention the Human Mutants created.6
Susan’s Jab related research
Her name varies with marital status, Monarez, Coller-Monarez, and Coller.
She has a keen interest in Lethal Endotoxin Shock.
In 2000 while at Wisconsin she used PCR to study Macrophage response via Type A1 scavenger receptor to IFN-γ and the SR ligand lipotechoic acid (LTA), Maleylated Bovine Serum Albumin, Polydeoxynucleotide Poly dI:dC and Endotoxin.7
Here is her experiment stimulating TNF-a protein production with Endotoxin (LPS) in comparison to LTA.

Fig. 5. TNF-a protein production is detectable after activation through the SR. RAW264.7 cells were stimulated with the SR ligands poly d[I:C], mBSA, or LTA for 6 h at 37°C, either alone (A) or after initial priming with IFN-g at 20 U/mL for 24 h (B). Cell-free supernatant fluids obtained by centrifugation were assayed for TNF-a levels by ELISA
As I pointed out, her use of the Poly dI:dC should probably be reinvestigated due to the likely Endotoxin contamination.8
In 2001 she published more research citing Endotoxin lethality papers.9
Also in 2001 she published work on the very nasty parasite Trypanosoma brucei rhodesiense surface glycoproteins.1011
In 2003 she published another useful paper12 that shows she has expertise in Endotoxin and resultant Cytokine Storm via Macrophages.
The abstract reads:
Macrophages are centrally involved in the host immune response to infection with Trypanosoma brucei rhodesiense, a protozoan parasite responsible for human sleeping sickness in Africa. During trypanosome infections, the host is exposed to parasite-derived molecules that mediate macrophage activation, specifically GPI anchor substituents associated with the shed variant surface glycoprotein (VSG), plus the host-activating agent IFN-gamma, which is derived from activated T cells and is essential for resistance to trypanosomes.
In this study, we demonstrate that the level and timing of exposure of macrophages to IFN-gamma vs GPI ultimately determine the macrophage response at the level of induced gene expression. Treatment of macrophages with IFN-gamma followed by GIP-sVSG (the soluble form of VSG containing the glycosylinositolphosphate substituent that is released by parasites) stimulated the induction of gene expression, including transcription of TNF-alpha, IL-6, GM-CSF, and IL-12p40. In contrast, treatment of macrophages with GIP-sVSG before IFN-gamma stimulation resulted in a marked reduction of IFN-gamma-induced responses, including transcription of inducible NO synthase and secretion of NO. Additional experiments revealed that the inhibitory activity of GIP-sVSG was associated with reduction in the level of STAT1 phosphorylation, an event required for IFN-gamma-induced macrophage activation. These results suggest that modulation of specific aspects of the IFN-gamma response may be one mechanism by which trypanosomes overcome host resistance during African trypanosomiasis.
In 2005 at Stanford she published on another parasite Toxoplasma gondii.1314
I will hunt for more of her publications related to Biowarfare, Viruses and Jabs.
Please let me know if you find some.
Trump nominates Enterotoxin, Anthrax and Nuclear Bomb Mass Killing expert Gerald Parker

Anthrax Jab developer and Enterotoxin expert assessing use of scarce resources after deployment of Nuclear Weapons for Genocide, fully understanding the Cancer effects in survivors, is a logical choice for Jab Pusher Trump. You can find him on X.
Nuclear Submarine Hazard in Western Australia - Have Citizens been issued Iodide Tablets ?

10 September 2024 was a big day in the history of Australian War Mongering.
Fauci the Endotoxin expert studied Individual Jab Susceptibility from 1974

I was talking to my friend a couple of days ago about the value of tracing research outputs of individuals involved in mass Jabbing and their detailed knowledge of Endotoxin Harms.
https://2024.worldmedicalinnovation.org/speaker/susan-monarez-phd/
C. Norman Coleman, Ann R. Knebel, John L. Hick, David M. Weinstock, Rocco Casagrande, J. Jaime Caro, Evan G. DeRenzo, Daniel Dodgen, Ann E. Norwood, Susan E. Sherman, Kenneth D. Cliffer, Richard McNally, Judith L. Bader, Paula Murrain-Hill. 2011. Disaster Medicine and Public Health Preparedness. S13-S19.
Mutant people in Brazil with Frame Shifted DNA caused by Cesium Gamma Radiation

Lunatics across the nation are sitting by quietly as a range of Politicians with absolutely no Science training commit us to receiving AUKUS Military Nuclear Waste and expanding the number of Nuclear Reactor Disasters in the making.
Donna M. Paulnock, Karen P. Demick, and Susan P. Coller. 2000. Analysis of interferon-γ-dependent and -independent pathways of macrophage activation. https://jlb.onlinelibrary.wiley.com/doi/abs/10.1002/jlb.67.5.677
Poly(I:C) viral dsRNA mimic studies invalidated by Endotoxin Contamination

Readers are aware that I always look at the Materials and Methods section of papers to see where the reagents were sourced, and this led me to write about Endotoxin invalidating many Covid19 “Spikeopathy” studies of the Coronavirus and Jabs that encode synthetic Spike.
Susan P. Coller, Donna M. Paulnock. 2001. Signaling pathways initiated in macrophages after engagement of type A scavenger receptors. https://jlb.onlinelibrary.wiley.com/doi/10.1189/jlb.70.1.142
https://en.wikipedia.org/wiki/Trypanosoma_brucei
Donna M. Paulnock and Susan P. Coller. 2001. Analysis of macrophage activation in African trypanosomiasis. https://jlb.onlinelibrary.wiley.com/doi/10.1189/jlb.69.5.685
Susan P Coller, John M Mansfield, Donna M Paulnock. 2003. Glycosylinositolphosphate soluble variant surface glycoprotein inhibits IFN-gamma-induced nitric oxide production via reduction in STAT1 phosphorylation in African trypanosomiasis. https://journals.aai.org/jimmunol/article/171/3/1466/966/Glycosylinositolphosphate-Soluble-Variant-Surface
https://en.wikipedia.org/wiki/Toxoplasma_gondii
Peter J Bradley, Chris Ward, Stephen J Cheng, David L Alexander, Susan Coller, Graham H Coombs, Joe Dan Dunn, David J Ferguson, Sanya J Sanderson, Jonathan M Wastling, John C Boothroyd. 2005. Proteomic analysis of rhoptry organelles reveals many novel constituents for host-parasite interactions in Toxoplasma gondii. https://www.jbc.org/article/S0021-9258(20)79014-9/fulltext