
Preprint: Evaluation of Febrile Seizure Risk Following Ancestral Monovalent COVID19 mRNA Vaccination Among U.S. Children Aged 2-5 Years.
Preprint: Evaluation of Febrile Seizure Risk Following Ancestral Monovalent COVID19 mRNA Vaccination Among U.S. Children Aged 2-5 Years.
LNP: DNA Plasmid/SPIKE/LPS (Endotoxin): cGAS GAMP STING Activation


What are the signs and symptoms of a febrile convulsion?
The symptoms of febrile convulsions include:
loss of consciousness (black out)
twitching or jerking of arms and legs.
breathing difficulty.
foaming at the mouth.
going pale or bluish in skin colour.
eye rolling, so only the whites of their eyes are visible.
”Febrile seizures are common in the first five years of life, and many factors that increase seizure risk have been identified. Initial evaluation should determine whether features of a complex seizure are present and identify the source of fever.
Routine blood tests, neuroimaging, and electroencephalography are not recommended, and lumbar puncture is no longer recommended in patients with uncomplicated febrile seizures.
In the unusual case of febrile status epilepticus, intravenous lorazepam and buccal midazolam are first-line agents.
After an initial febrile seizure, physicians should reassure parents about the low risk of long-term effects, including neurologic sequelae, epilepsy, and death.
However, there is a 15 to 70 percent risk of recurrence in the first two years after an initial febrile seizure. This risk is increased in patients younger than 18 months and those with a lower fever, short duration of fever before seizure onset, or a family history of febrile seizures.”

Febrile Seizures: Risks, Evaluation, and Prognosis
*************************************************************************************************************
(get used to the photo below. It will be very important the moment someone does a study on it. Perhaps somewhere on the East Coast—where they have palm trees.)

Let’s review key points and then roll right into the mechanisms.
(an Epoch article led me here—thank you)
The study in question:
Evaluation of Febrile Seizure Risk Following Ancestral Monovalent COVID19 mRNA Vaccination Among U.S. Children Aged 2-5 Years Forshee et al. 2024
The study begins with the key points:
”Key Points Question: Among children aged 2-5 years, is the risk of febrile seizure elevated immediately following monovalent COVID-19 mRNA vaccination compared with a later period after vaccination?
Findings: In this self-controlled case series that included participants aged 2-5 years from three commercial insurance databases, the incidence rate ratio of febrile seizures was significantly elevated in the 0-1 days following mRNA-1273 administration.
The study authors go on to state that the absolute risk was small.
”Importance The United States Food and Drug Administration noted a potential safety concern for seizure in children aged 2-5 years receiving the ancestral monovalent COVID-19 mRNA vaccines.
Objective To evaluate febrile seizure risk following monovalent COVID-19 mRNA vaccination among children aged 2-5 years.
Design, Setting, and Participants The primary analysis evaluated children who had a febrile seizure outcome in the 0-1 days following COVID-19 vaccination. A self-controlled case series analysis was performed in three commercial insurance databases to compare the risk of seizure in the risk interval (0-1 days) to a control interval (8-63 days). Exposure Receipt of dose 1 and/or dose 2 of monovalent COVID-19 mRNA vaccinations.
Main Outcomes and Measures The primary outcome was febrile seizure (0-1 day risk interval).
Analysis A conditional Poisson regression model was used to compare outcome rates in risk and control intervals and estimate incidence rate ratios (IRR) and 95% confidence intervals (CIs).
Metanalyses were used to pool results across databases.
Results:
The primary meta-analysis found a statistically significant increased incidence of febrile seizure, in the 0-1 days following mRNA-1273 vaccination compared to the control interval (IRR: 2.52, 95% CI: 1.35 to 4.69, risk difference (RD)/100,000 doses = 3.22 (95%CI -0.31 to 6.75)). For the BNT162b2 vaccination, the IRR was elevated but not statistically significant (IRR: 1.41, 95%CI: 0.48 to 4.11, RD/100,000 doses = -0.25 (95%CI -2.75 to 2.24).
Among children aged 2-5 years, the analysis showed a small elevated incidence rate ratio of febrile seizures in the 0-1 days following the mRNA-1273 vaccination”
Let’s hop out of that study and do math.
We know that at least 5 billion people total got the “vaccine” on the planet—at least one dose.
When calculating risk in statistics, in epidemiology or public health, the population at risk refers to the individuals who are susceptible to the outcome of interest within a defined population.
In the case of febrile seizures following “vaccination”, the population at risk would typically be children who are eligible to receive the vaccine and are susceptible to experiencing febrile seizures. This population would include children within a certain age range, usually those who are young enough to be at risk for febrile seizures.
Therefor, we are talking the global population of all persons 5 and under.
Math (is this correct?):
Assumptions:
Population under age 5: 656,640,181
Location: World
Year: 2023
Source: https://data.unicef.org/how-many/how-many-children-under-18-are-in-the-world/
Percentage of Population in Age Group 0-5 Years:
Moderna :mRNA-1273 “Vaccination”:
Percentage of Risk for mRNA-1273 = (3.22/100,000)×656,640,181=21,166.15
That’s a possibility of 21,166.15 children under the age of five developing febrile seizure from Moderna “vaccine” based on population estimates and the math presented in the study, statistically speaking.
BNT162b2 “Vaccination”:
Percentage of Risk for BNT162b2 = (−0.25/100,000)×656,640,181=−1,641.6
Interesting number on this one.
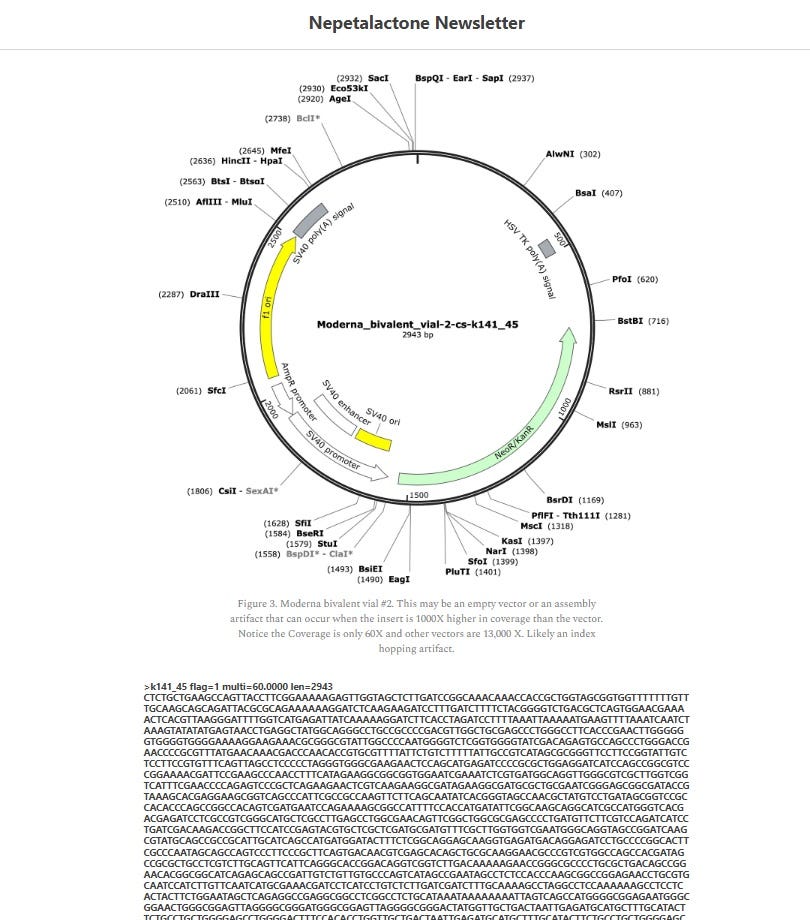
This is interesting from what we know of the contamination issues with DNA plasmid, although that is not the only key marker at play.
It is known that if we are looking at impacts on the cGAS STING pathway on seizures (I’ll post the stroke one next), then there is a chance that spike protein, DNA plasmid pieces, AND DNA from bacteria (Endotoxin LPS) would be activating the cGAS STING pathway.
If one were to base the activation by concentration of DNA plasmid pieces alone, there is data by Mckernan et al that the Moderna vials had less contamination compared to Pfizer when it came to DNA plasmid pieces. however, the amount of endotoxin (Geoff might want to chime in if he has numbers) on the LPS from the E coli used.
Also, one would look at the number of spike protein produced by each “brand”, and if Moderna had higher amounts of spike produced, in combination with potential LPS, one would assume the higher number from Moderna over Pfizer might be correlated.
If it were going to occur, this would be the mechanisms:
Mechanisms for cGAS STING in relation to febrile seizures:
Viral DNA (SPIKE PROTEIN):
Within the cytoplasm, the DNA from the virus/SPIKE PROTEIN is detected by the cyclic GMP-AMP synthase (cGAS).
After binding to viral DNA/SPIKE, cGAS catalyzes the synthesis of cyclic GMP-AMP (cGAMP) from ATP and GTP.
The generated cGAMP serves as a second messenger that binds to and activates the Stimulator of Interferon Genes (STING) protein—localized on the endoplasmic reticulum membrane.
Activated STING initiates downstream signaling cascades, producing type I interferons and other cytokines.
Bacterial DNA and LPS Endotoxin:
Bacteria, upon invasion or phagocytosis by immune cells, can release their DNA into the host cell's cytoplasm. Bacterial cell wall components like lipopolysaccharide (LPS) endotoxin can trigger immune responses.
Bacterial DNA/LPS endotoxin in the cytoplasm activates the cGAS-STING pathway.
Detection of bacterial DNA or LPS by cGAS makes cGAMP, subsequent activation of STING, and the induction of innate immune responses.
Exogenous DNA and DNA Plasmid Pieces:
Fragments of Plasmid DNA can trigger the cGAS-STING pathway.
DNA plasmid pieces, may inadvertently activate cGAS upon introduction into host cells.
Detection of exogenous DNA fragments by cGAS results in the synthesis of cGAMP and subsequent activation of STING, leading to immune activation.
Implications for Febrile Seizure Activation:
Febrile seizures, which occur in young children during episodes of fever, have been associated with rapid increases in body temperature, often due to viral or bacterial infections.
Activation of the cGAS-STING pathway by SPIKE, DNA PLASMID PIECES, and/or bacterial DNA during infection-induced fever can contribute to the pathogenesis of febrile seizures.
The release of inflammatory cytokines and chemokines downstream of cGAS-STING activation may lead to neuronal hyperexcitability and seizure activity.
Detailed mechanism once cGAS STING is activated of inducing seizure activity:
Inflammatory Cytokines and Chemokines:
Activation of the cGAS-STING pathway in response to viral, bacterial, or exogenous DNA triggers a cascade of signaling events that culminate in the production and release of inflammatory cytokines and chemokines.
Inflammatory cytokines such as interleukin-1 beta (IL-1β), tumor necrosis factor-alpha (TNF-α), and interleukin-6 (IL-6), as well as chemokines like CXCL10 (also known as IP-10), are among the key mediators released in response to cGAS-STING activation.
These cytokines and chemokines are involved in both immune responses, and inflammation.
Neuronal Hyperexcitability:
Inflammatory cytokines and chemokines released during immune activation alter neuronal excitability and synaptic transmission within the central nervous system.
IL-1B, TNF-α, and IL-6, modulate synaptic strength and plasticity, nd neuronal excitability, by modulating ion channel activity and synaptic receptor expression.
Chemokines such as CXCL10 can also influence neuronal function by directly acting on neurons or by attracting immune cells that release additional inflammatory mediators. Excessive or dysregulated release of these inflammatory molecules in response to cGAS-STING activation may lead to aberrant neuronal firing patterns associated with seizures.
Theses effects most likely involve complex interactions within the CNS, including neurons, glial cells, and infiltrating immune cells all in combination.
What this means is, the beginning of the process involves spike protein/viral DNA, bacterial DNA (endotoxin/LPS), and plasmid DNA to activate the cGAS GAMP STNG pathway. This activation engages the innate immune system in ways that direct the immune system to be recruited to the area this is occurring, and in this case, the brain. The parts of the brain then become inflamed, and the cGAS GAMP STING may lead to neuronal hyperexcitability and seizure activity through the release of cytokines and chemokines.
This is all happening in the brain. And in this case, the brain of a baby.
References:
https://www.mdpi.com/2218-273X/10/10/1437
https://www.frontiersin.org/journals/immunology/articles/10.3389/fimmu.2023.1235590/full
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10433641/
https://journals.physiology.org/doi/full/10.1152/jn.00848.2018
https://www.tandfonline.com/doi/full/10.1080/02656736.2020.1868582#:~:text=These%20results%20show%20that%20febrile,of%20the%20cGAS%2DSTING%20pathway.